Retatrutide,
done properly.
Most research-grade reta vials go cloudy, lose potency, or arrive contaminated. Ours doesn't — because the formulation, the BAC water, and the cartridge were all engineered together. Here's what makes the difference, and how to use the cart from first dose to last.
Why our reta is better
Retatrutide is a lipidated peptide — it has a fatty acid tail bolted onto the protein backbone, exactly like semaglutide. That tail is what gives reta its week-long half-life, but it's also why most research-grade reta vials fail. The fatty tail wants to stick to glass walls, clump with other reta molecules, and crash out of solution the moment pH drifts off-target.
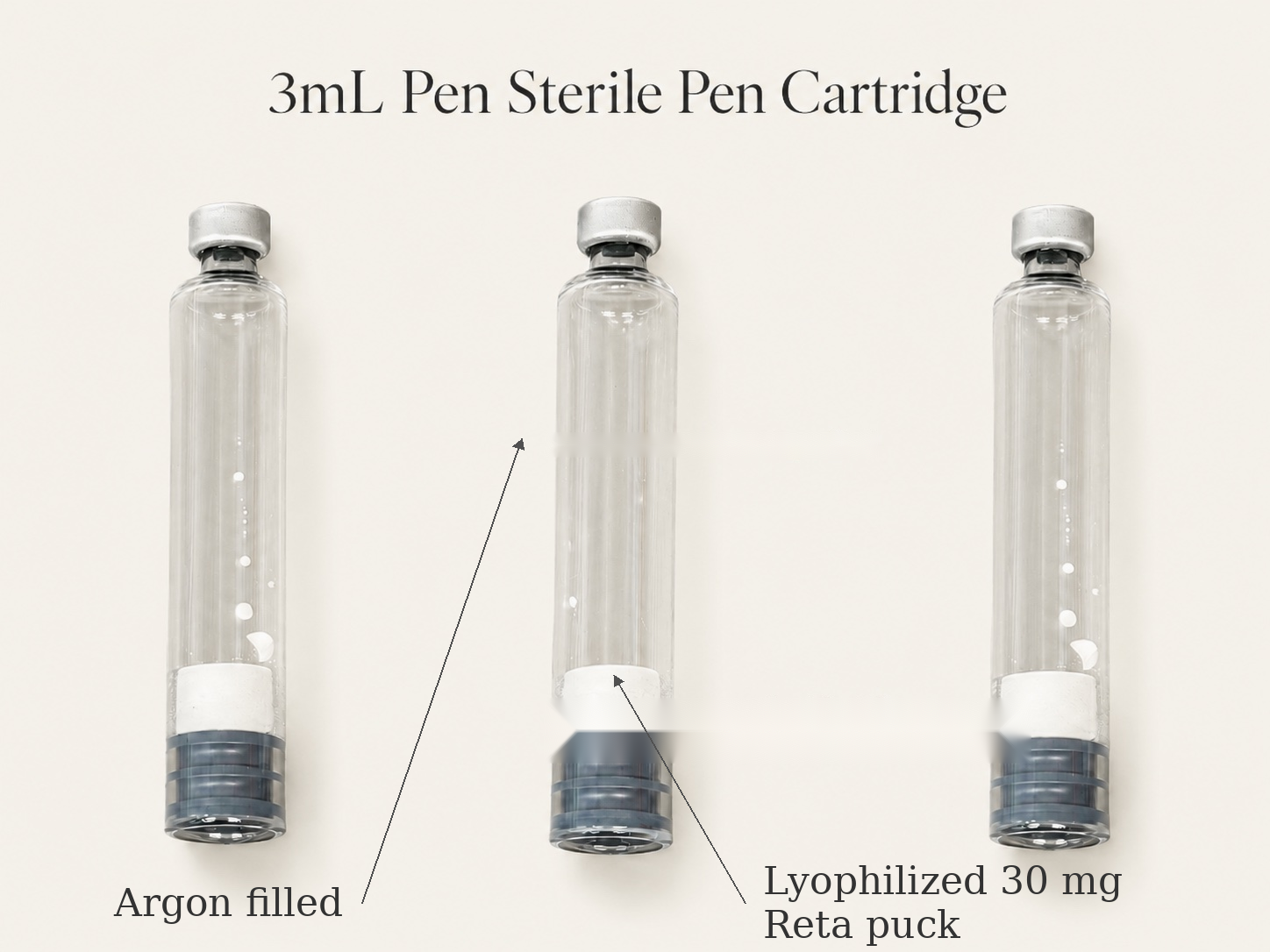
We formulated around every one of those failure modes. Our reta isn't just powder in a vial — it's a complete pharmaceutical-grade formulation with buffers, chelators, and a heavy trehalose lyoprotectant matrix baked directly into the lyophilized cake. When BAC water hits the cake, every stabilizing excipient activates in the same instant the peptide does.
The result: clear solution on contact, stable for the life of the cart. No cloudiness. No chunks. No "wait an hour and swirl harder."
Why our BAC water is better
BAC water seems simple — just sterile water plus 0.9% benzyl alcohol — and most vendors treat it that way. We don't. Our BAC is fluid-engineered for peptide reconstitution from the moment the vial is filled.
First: argon-flushed during fill. Same protocol as the cartridge itself. Room air never sits over the BAC water. That means zero dissolved oxygen entering your cart at reconstitution — the moment when the peptide is most vulnerable.
Second: argon-packed in the vial. Headspace above the BAC is pure argon, sealed at atmospheric pressure. The BA preservative handles bacteriostatic protection; the argon handles oxidation protection. Two layers, working at the same time.
Third — and this is the part nobody talks about — our BAC is pH-balanced to 5.8–6.0. Most BAC sits wherever benzyl alcohol's natural pH happens to land, which means every batch is slightly different and every reconstitution is a small experiment. Ours is deliberately tuned to a tight, predictable window — and that window matters for two completely different reasons.

For our reta: a clean 5.8–6.0 starting point lets our cake's buffer system reliably pull the final solution down to its target landing pH of 5.5. Other research-grade reta formulas don't have any cake buffer at all — so their final pH is whatever random number the BAC happened to be that day. Ours is engineered end-to-end.
For products that can't use pH buffers at all — copper peptides like GHK-Cu (the active ingredient in KLOW) physically cannot tolerate histidine, EDTA, or phosphate buffers because those excipients either chelate the copper or strip it out of the peptide entirely. For these formulations the BAC water is the only pH control there is. Our 5.8–6.0 spec lands them safely in the copper-stable range every single time. Standard unmonitored BAC can put them anywhere from pH 4 to pH 7, and the copper falls out of the complex on either extreme.
Why pen cartridges are better
A traditional vial sits there with the same headspace volume forever — every dose you pull, room air gets drawn back through the needle to replace what you took out. By the end of the vial, your last dose is sharing space with weeks of accumulated bacteria, oxygen, and dust nuclei. This is the single biggest reason reconstituted peptides degrade.
A pen cartridge works the opposite way. As the plunger advances with each dose, the air space shrinks instead of growing. By your last dose, there's almost no headspace at all — and what little exists has been steadily compressed and pushed out, not exchanged with the room.
Combine that mechanical advantage with how you reconstitute the cart in the first place — argon vents out, BAC water pushes in, never room air — and you get a sealed system from end to end. Bacteria physically cannot enter against the outward gas flow during reconstitution, and once sealed, the plunger compression keeps it that way.

Why ours is still working when theirs is gone.
Reconstitution — your BAC goes into the cart
Each Reta-30 ships with a matched 1.8mL BAC water vial. You transfer all of that BAC into the pen cartridge. The cart then dispenses against a 1.6mL working volume — the extra 0.2mL fills the dead space inside the pen mechanism so every dialed unit lands in the tissue, not lost in the device.


Pushing the air out — first prime & every dose
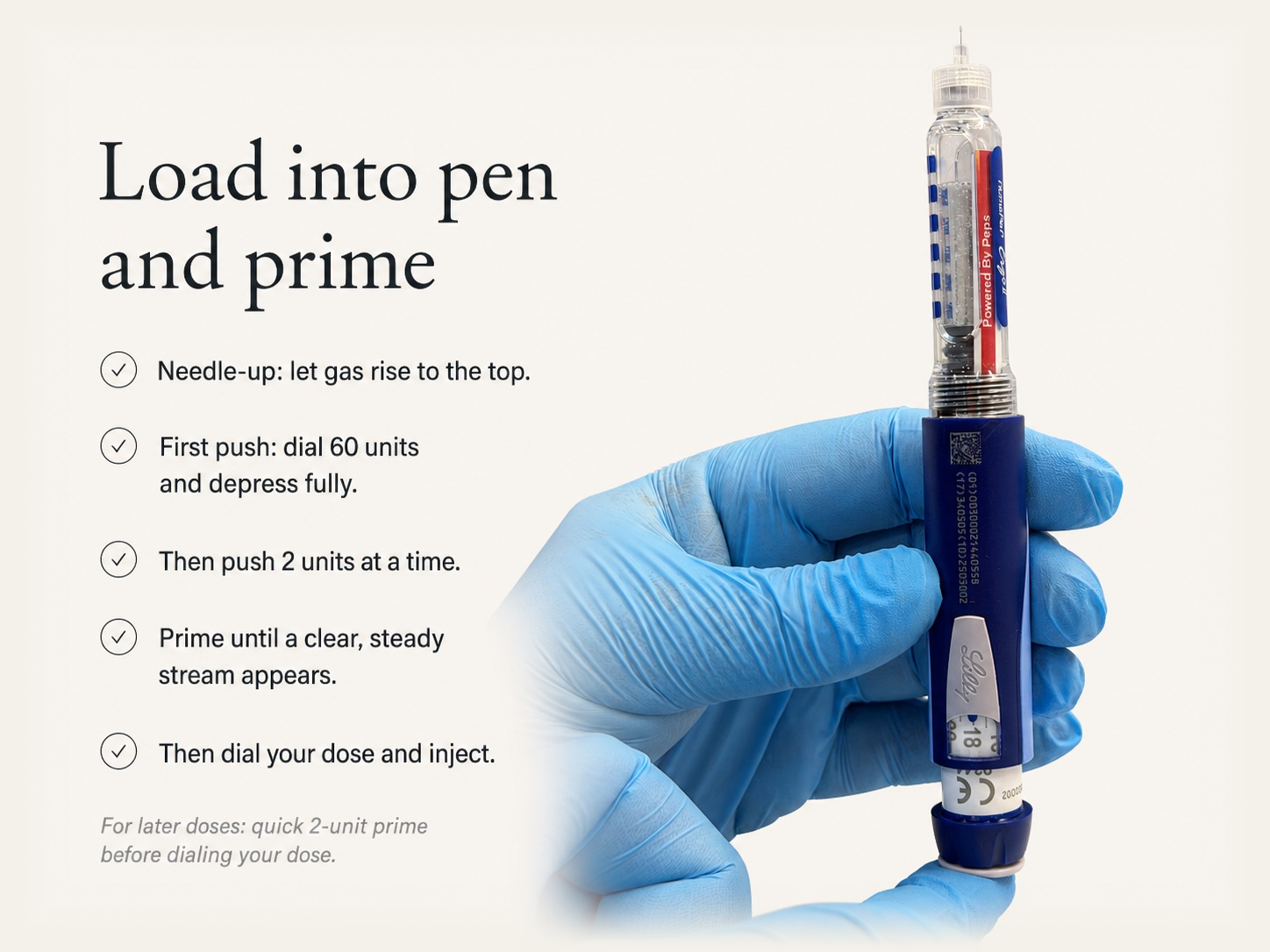
After reconstitution, a small pocket of argon mixed with a bit of dissolved gas will sit at the top of the cart. You want to push as much of it as possible out before your first dose. This shrinks the headspace for the rest of the cart's life — less air to absorb into solution, less surface area for the peptide to lose to oxidation over weeks of use.
The good news: priming the pen handles this automatically. Each prime push moves the plunger forward, compresses the gas pocket, and vents it through the needle. Once it's out, it can never get back in.
- Hold the pen needle-up so any gas pocket migrates to the top, near the needle.
- First push: dial a full 60 units and depress fully. Because we know exactly 1.8mL of BAC went into the cart, a 60-unit push is safe and will clear most of the headspace gas in one shot.
- After that, slow down. Dial 2 units at a time, push fully, and watch the needle tip. You'll see nothing at first — that's normal, you're still pushing gas out.
- Keep going 2 units at a time until a clear, steady stream of fluid shoots out of the tip. That stream is your confirmation — fluid is at the needle, gas is gone.
- Cart is purged. Dial your dose and inject.
- Every subsequent dose, do a quick 2-unit prime needle-up before dialing your real number. Confirms the line is clean, keeps the cart sharp through the last dose.
Dosage — Reta-30 monthly titration
| Phase | Weekly dose | Pen units | Volume |
|---|---|---|---|
| Month 1 | 2 mg | 11 | 0.11 mL |
| Month 2 | 4 mg | 21 | 0.21 mL |
| Month 3 | 6 mg | 32 | 0.32 mL |
| Month 4 · hold | 8 mg | 43 | 0.43 mL |
| — glucagon activity kicks in around 8 mg · hold here, assess fat-loss response before climbing — | |||
| Optional · if needed | 10 mg | 53 | 0.53 mL |
| Optional · ceiling | 12 mg | 64 | 0.64 mL |